
Table of Contents
To VAX or NOT TO VAX? That Is The Question!
Never in the World’s history has such a seemingly simple answer to a question overwhelmingly divided friends, families, and indeed nations.
I’m a Melbourne University strongly educated mathematician & scientist, ex-military pilot, father of teenagers & blogger.
.
I am a fierce proponent of a balanced view & educated CHOICE.
.
My take in regard to Covid-19 vaccination is NOT political, – I’ve already had Covid19 so I don’t need vaccination. I’m neither PRO nor CON vaccination, I believe in choice – but educated choice. I have no vaccine company shares & might make beer money at best from any advertising revenue from the website this is published on.
I’m writing this because there is so much disinformation out there but unlike me, most simply do not have the time, or expertise in research, to sift through the noise. Right now – I simply have nothing better to do…
Data is from government sources or with [REF].
ONS UK, CDC USA, TGA Australia, Israel, Canada & W.H.O.
.
I always agree that we should listen to experts. That doesn’t mean you have to talk to them in person, however. I have left references for all the research acquired from experts worldwide.
I do NOT believe in conspiracy theories, but I do believe power and money can often obscure the real truth.
As such I’ve included some figures at one end of the scale where deaths have been reported but officially discounted as unrelated. I’ll call them the ‘Unlikely but just in case’ figures. (UF)
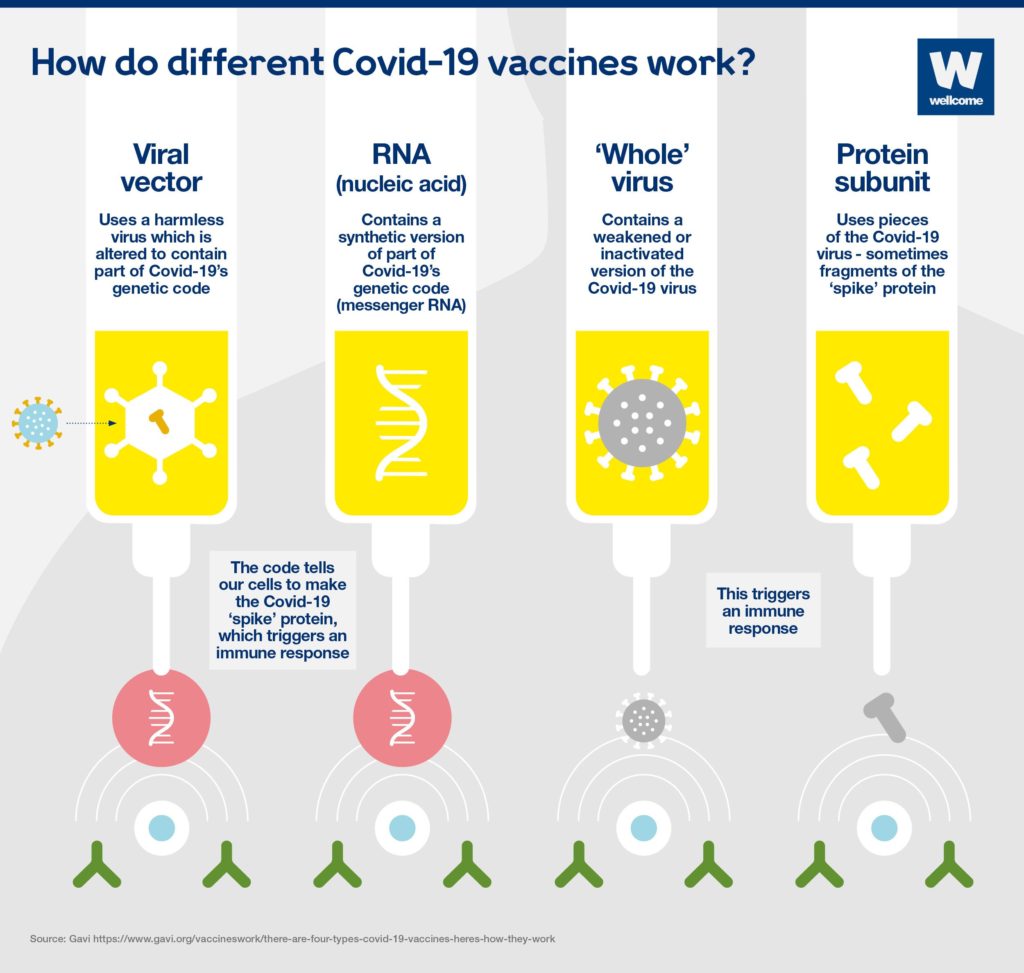
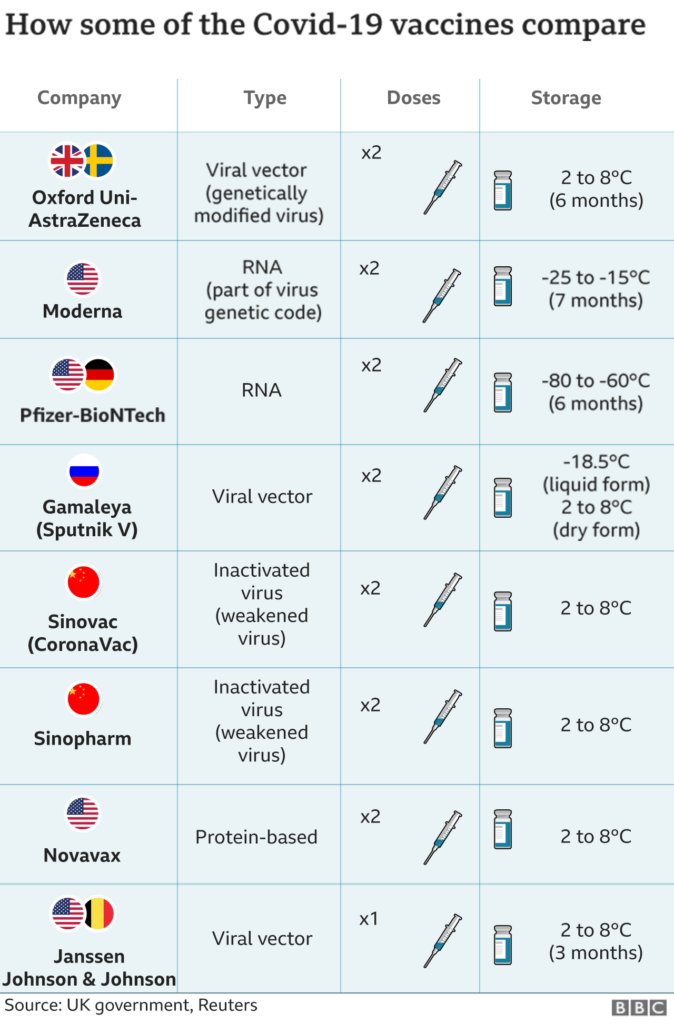
Every vaccine is slightly different, this post has researched AstraZeneca, Pfizer, Moderna, and Johnson & Johnson. These are the most common vaccines being used in the UK, USA, Australia, Canada, Israel, and Europe.
The author is Not a Doctor. This post is a GUIDE ONLY specifically in relation to AGE, published odds of survival, and relevant arguments to consider. SEEK PROFESSIONAL MEDICAL ADVICE in relation to your own health circumstances and vaccine suitability
Sidenote: *Given the evidence, I am somewhat bewildered as to many (not all) governments’ policies, particularly in relation to young children & vaccination. This article may shed light on the reasons why.
“You never want a serious crisis to go to waste.”
Table of Contents
Firstly – If Over 65 y/o All Research Suggests It’s Such A No Brainer There’s No Point In Much Discussion.
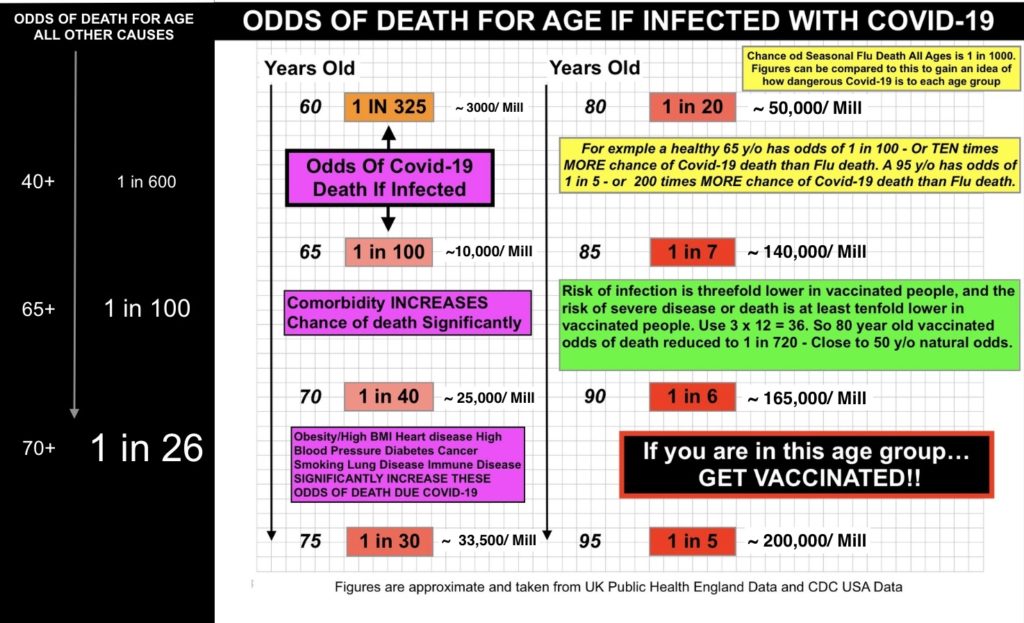
ODDS OF DEATH/ AGE DUE COVID-19 > 60 Y/O
.
If in this age group and you have a strong desire to live – Get Vaccinated – NOW
Covid-19 kills 1 of 20 healthy people on average in that age group. Those odds get significantly WORSE if you are obese/ high BMI or managing high blood pressure, diabetes, heart or lung disease, cancer, or most other comorbidities. Chances are you WILL be exposed to Covid-19 in the next few years. The flu by comparison kills 1 in 1000 ( all age groups). Even If you don’t fear the flu at your age – simple maths says your chances are abysmal against Covid-19 unless you get vaccinated.
The risk of death/ serious adverse reaction from the vaccines is 45.5*- 121/mill. For a 65 yo chance of Covid -19 death if unvaccinated is 10,000/ mill and for a 95 yo 200,000/mill. [*See Adverse effects section]
.
Slide C1
The risk of death/ serious adverse reaction from the vaccines is 27.5 – 121/mill. For a 65 yo chance of CVD death if unvaccinated is 10,000/ mill and for a 95 yo 200,000/mill.
Slide C1A
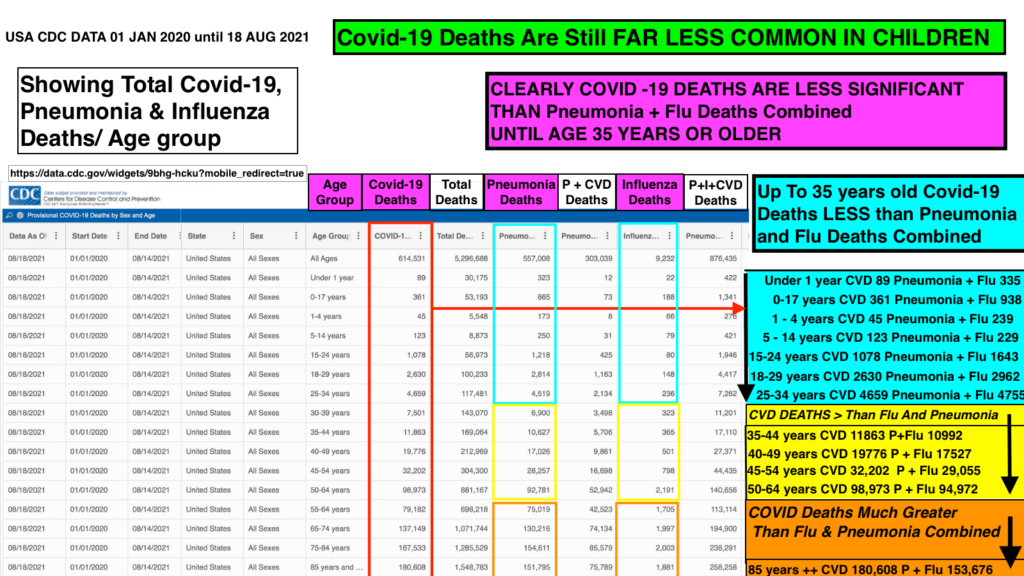
Covid-19 Deaths are uncommon in children.
The Benefits Of Vaccination – Latest Estimates Taking Into Account ‘Delta’ Variant.
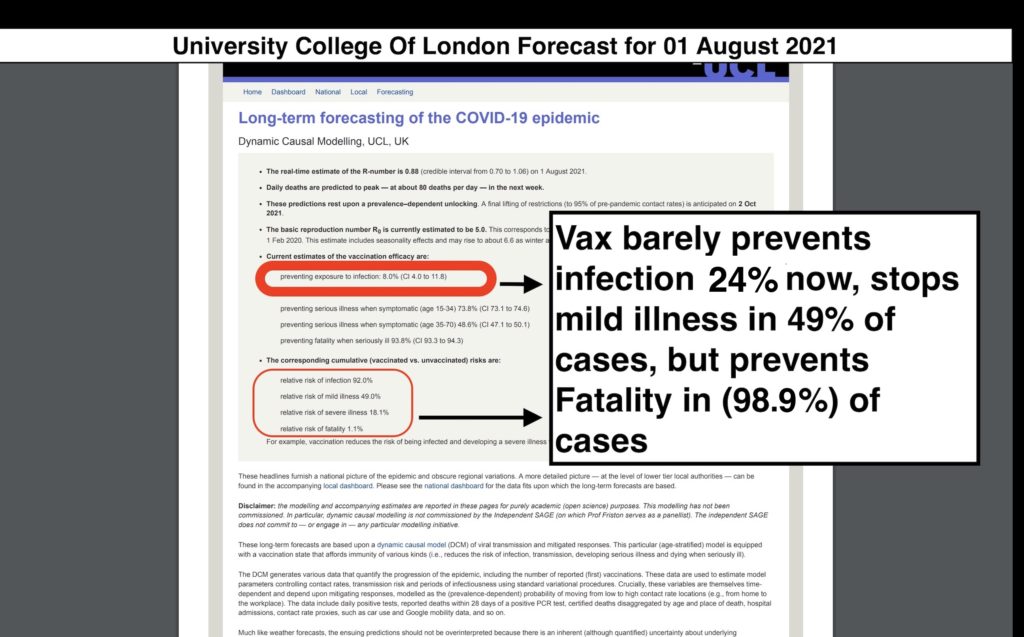
- Vaccination – reduces the chance of getting an infection by around 24%. [UCL] See Slide D2 for Chance of Symptomatic Infection
- Vaccination reduces the chance of severe disease and death by around 98%.
- Importantly once vaccinated, one can still transmit Covid-19 after infection to others, albeit for a slighly lesser time period. .
UK Public Health documents indicate the resultant risk of severe disease or death is initially around ten to twelve times lower on average for all of these vaccines.
Latest World Data – Disturbing…
Latest -Aug 2021-World Data Shows
.
1)Vax Booster Needed After 6 Months.
2) DELTA Variant Is Causing Far More Breakthrough Infections In The Fully Vaxed. There is far less protection against infection with Delta.
3) Fully Vaxed Can Spread Delta As Easily As Unvaxed (Herd Immunity Unlikely)
4) Vax Remains Largely Effective Against Death/ Severe Disease For ~ 6 Months
5) Delta Far More Contagious But Unlikely More Deadly
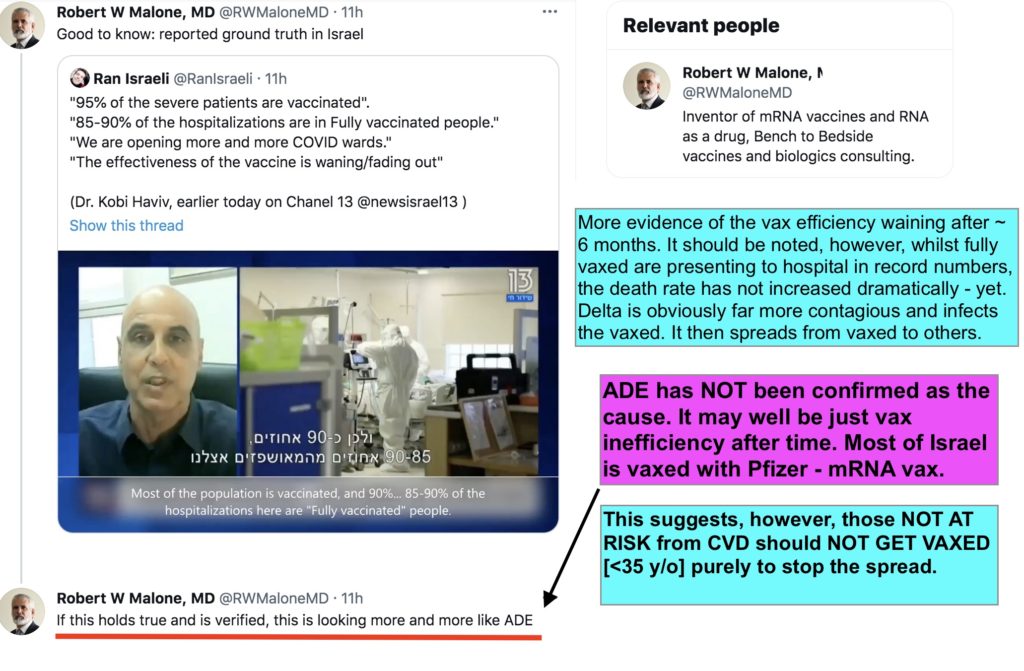
The Israeli Public Health Director on Aug 01, 2021, said they’ve seen “increased hospitalization of severe & critical cases in fully vaxed > 60 year olds”

Covid Vaccines: The Good, The Bad, The Ugly Reports: [Updated: Aug 06, 2021]
*In the UK, which has primarily used the AstraZeneca DNA adenovector vaccine, the latest estimate by researchers at University College London indicates effectiveness against infection of only *23.7%
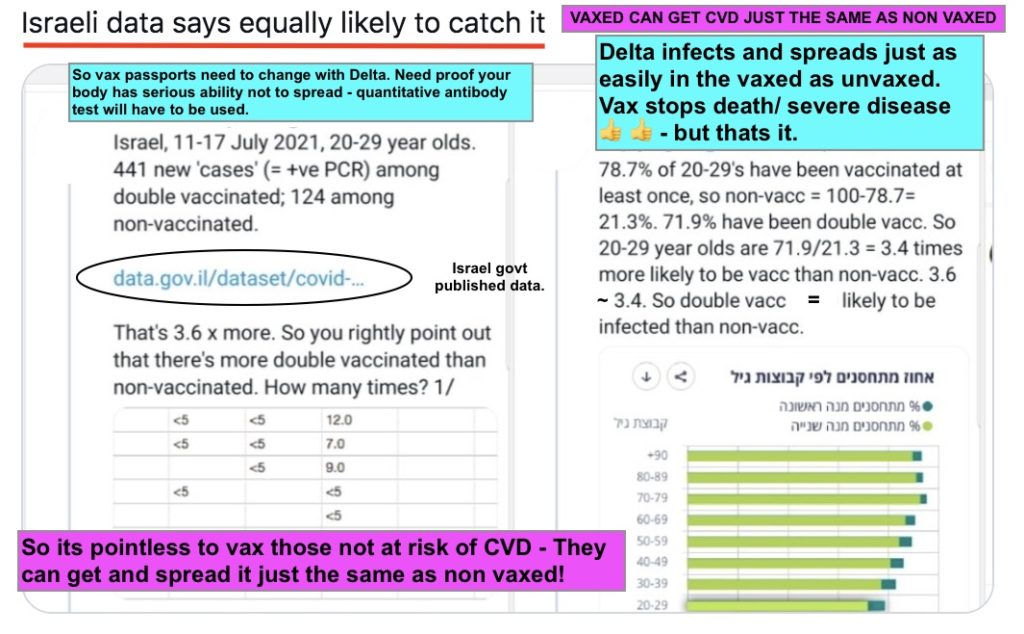
New data from Israel shows that “only 20%” of fully vaccinated people have infected others in public spaces. While authorities claim that this is a success, in reality, it is not any different from unvaccinated people, thus confirming almost zero effectiveness against infection and transmission.
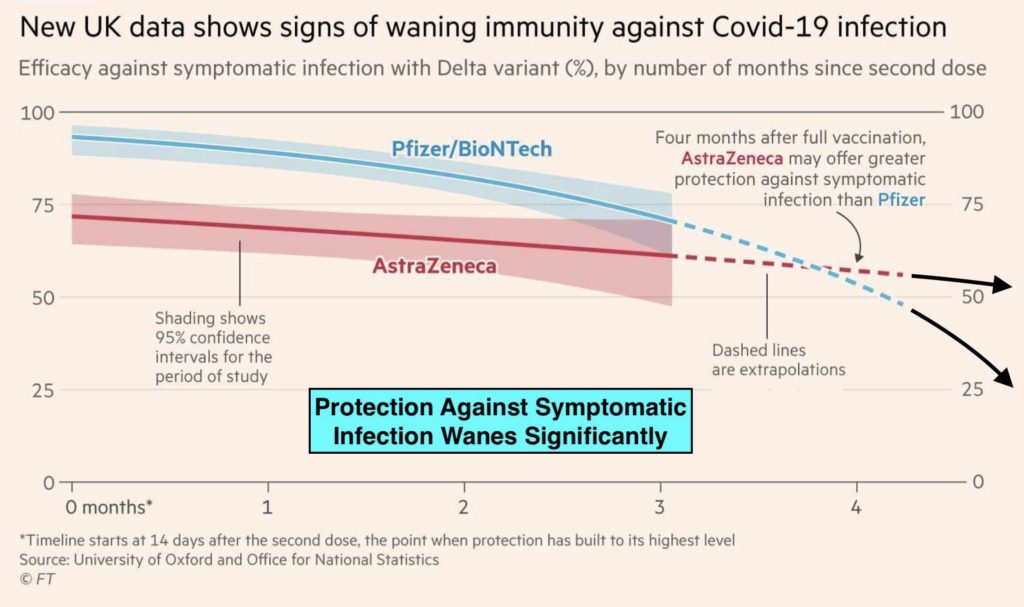
Slide D2 – Protection against Symptomatic Infection reduces significantly after 6 months.
The Washington Post, on 29 Jul 2021 reported USA CDC internal documents;
.
‘showing that vaccinated individuals infected with delta may be able to transmit the virus as easily as those who are unvaccinated.’
.
‘One of the slides states that there is a higher risk among older age groups for hospitalization and death relative to younger people, regardless of vaccination status. Another estimates that there are 35,000 symptomatic infections per week among 162 million vaccinated Americans.’
The document played a key role in revamped recommendations that call for everyone – vaccinated or not – to wear masks indoors in public settings in certain circumstances.
Increasing Evidence of
Breakthrough Infections.
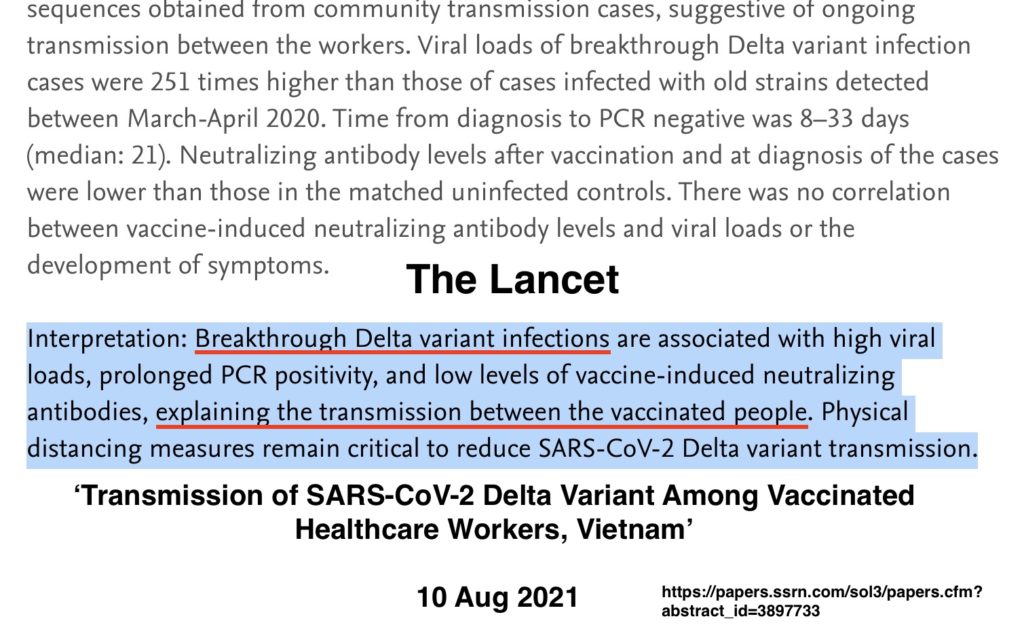
The Lancet article of 10 Aug 21, suggests that with Delta, the vaccinated could in fact become ‘Super Spreaders” with breakthrough infections. Note this is not yet peer-reviewed, so until then we should call it (UF)*
Slide D3
*Latest UCL update 5 Aug 2021 shows 23.7% reduction infection (Still far less than original)
It seems Delta can infect the vaxed almost as easily as non-vaxed. The great news is that: The vax still seems to protect against severe outcomes and death for up to 6 months.
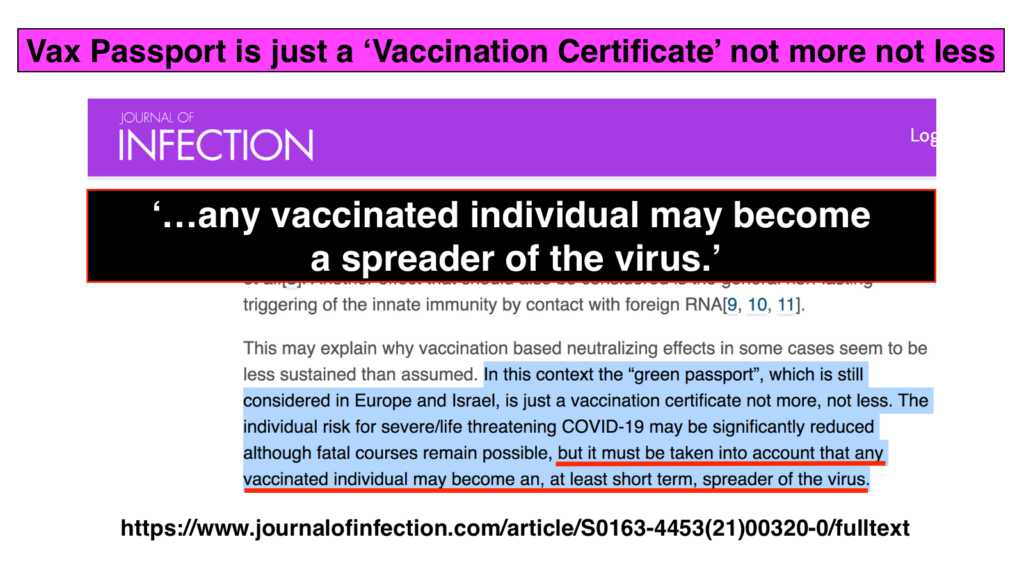
Journal of Infection article of 09 Aug 21 confirming Delta far more contagious and
Both Vaxed and Unvaxed CONTRACT AND SPREAD the virus. (CDC shows its not more deadly)
The very latest news from CDC USA, Israel, UK, Iceland and other highly vaxed countries is disturbing and has ramifications for vaxing younger age groups. See more in the Explanations section and Adverse Effects section.
The fact its effectiveness remains high for severe disease at least for a period of months means vaxing the old and unhealthy remains a:
‘No Brainer Do It Yesterday!’
‘To Vax or Not To Vax’ is easily resolved for those above 65 years old. The younger the age, however, the more complex the answer becomes.
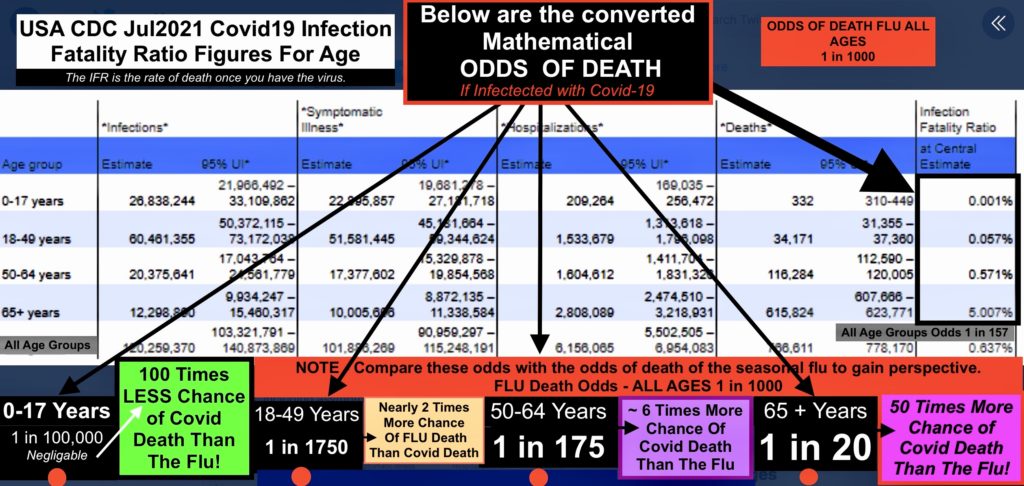
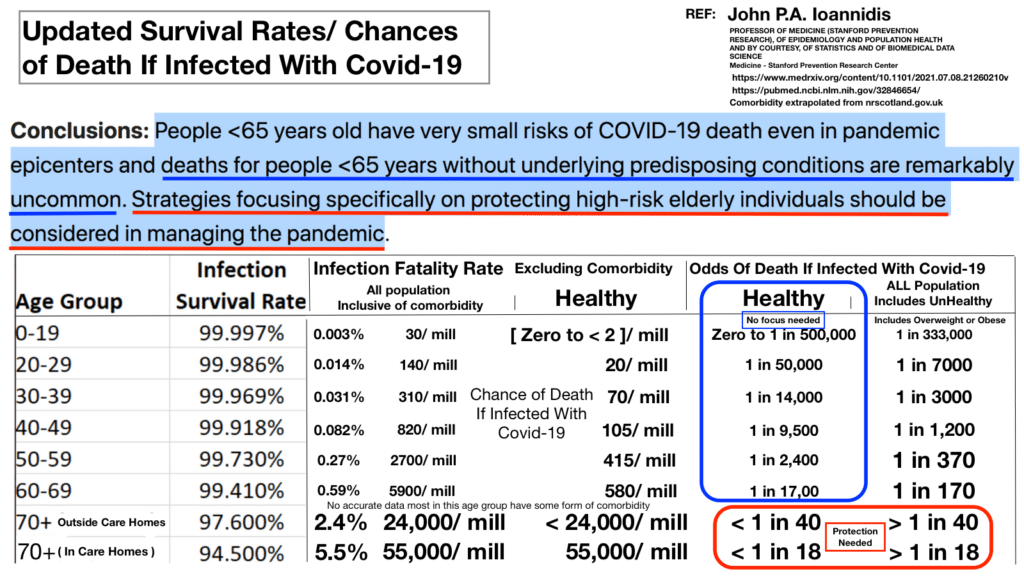
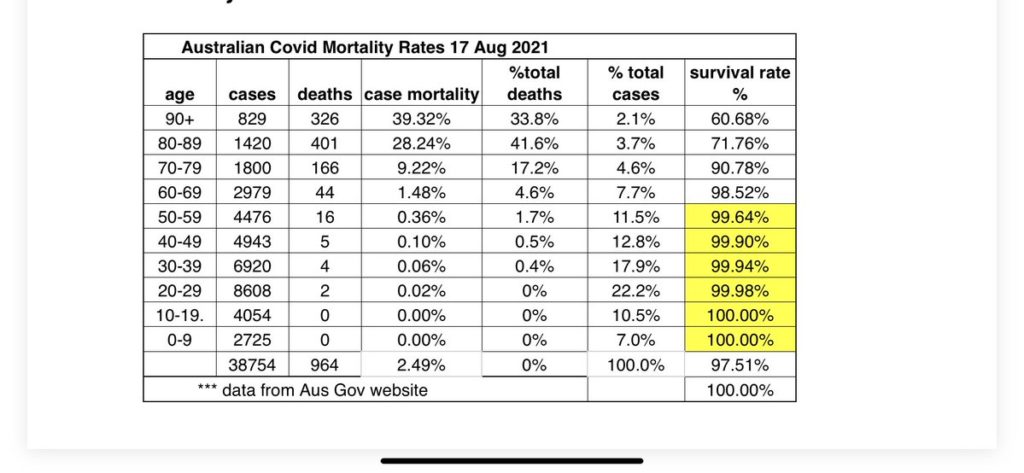
Below are the latest USA government CDC figures for Covid-19 (CVD) Infection Fatality Ratio (IFR) for age. The IFR is the rate of death once you are actually infected with the virus. I have converted them to simple ‘Odds of death’ if infected.
Odds of death of ‘1 in 20’, meaning for every 20 people who contract the virus, 1 will die on average.
Note this table separates and averages IFR into large age groups. The average odds agree however with the more detailed slides provided from UK Public Health data in charts C1 and C3 and C4.
Slide C2
Note that the latest John Hopkins research found that ZERO of the CDC *reported deaths under 17 y/o were in fact due to Covid-19, rather they were from comorbidity. This suggests the Odds of CVD death are closer to 1 in 500,00 – negligible for this age group. *Note also 37.5% US Pop Hispanic/ Black/ S Asian. Comorbidity & these risk factors reduce significantly the healthy population the conclusions of this article are based on.
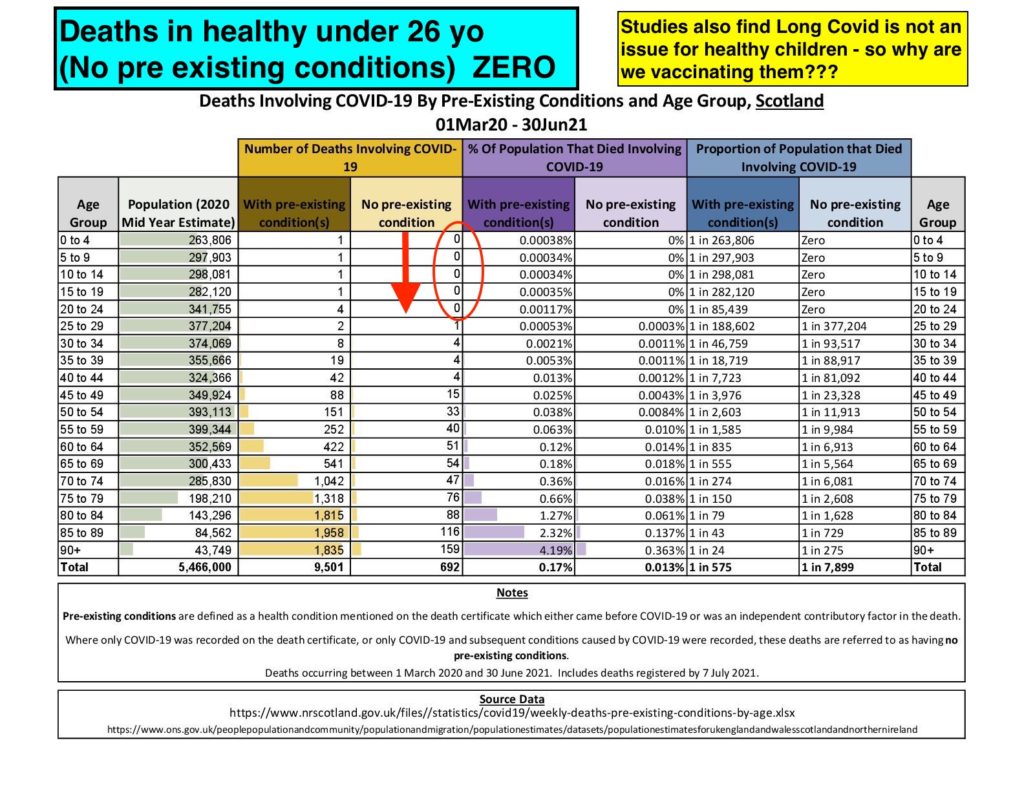
Slide C2A Scottish data shows Zero death in healthy under 26 yo for the entire pandemic
Slide C2B – Age and Comorbidity have a massive influence on survival chances
The Best Way To Use These ‘Covid-19 Odds Of Death’ Is To Compare Them To The ‘Odds Of Death’ Of The Seasonal Flu.
We are all familiar with the flu – we know it can be a nasty disease, but we don’t adjust our lives and livelihoods to prevent flu infection.
The flu odds of death remain at around 1 in 1000 for ALL AGE GROUPS.
The flu is nowhere near as discriminatory for age as Covid-19.
.
If the ‘Odds of death’ are SIGNIFICANTLY GREATER for Covid-19 than the flu (eg 1 in 100 or 1 in any number lower number than 1000) – then we probably should start taking precautions to prevent our own death. Vaccination (Vax) is one such precaution.
Similarly, if our ‘Odds of death’ are significantly LESS than the odds of death due to the flu (1 in a LARGER number than 1000), then we need not fear death from CVD more than we fear death from the flu. CVD Odds of death for a 42-year-old are around 1 in 1,750 for example. This means you have 1.75 times (almost two times) LESS chance of dying from CVD than the flu.
If you are a very healthy 42-year-old, vaccination at this age might be motivated more by preventing long Covid, severe disease, or attempting to stop the spread of CVD to your elderly parents or unhealthy friends.
To Vax or Not To Vax For Those Under 65
ODDS OF DEATH/ AGE DUE COVID-19 < 60 Y/O
Below slide – C3 presents a detailed summary of odds of death for age if infected with CVD for those up to 65 years of age.
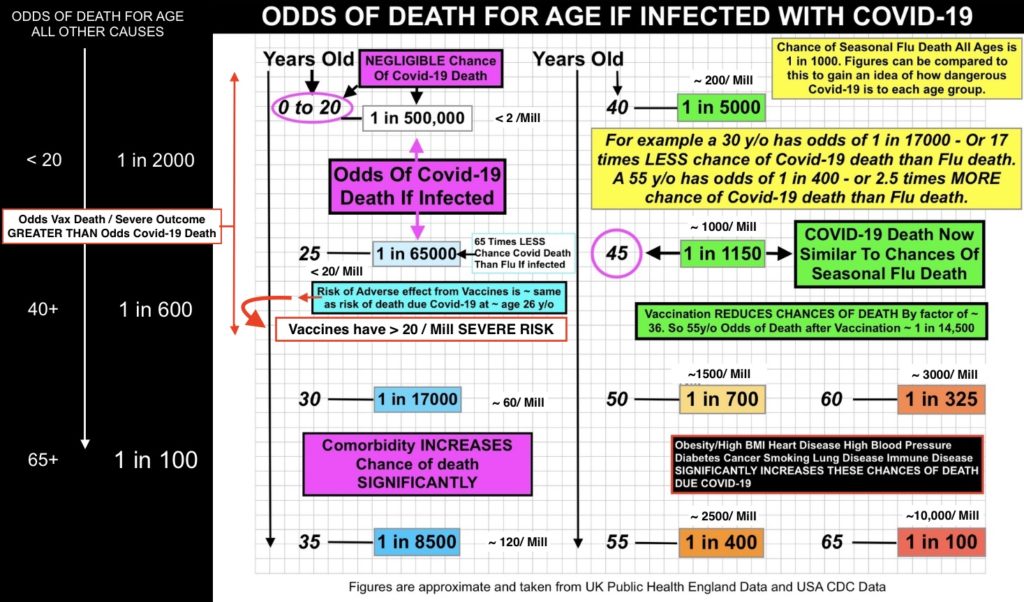
Slide C3
The chance of death/ severe outcome due to vax is 27.5* *Add 18/ mill to account for Pericarditis – 121/mill. [See Adverse Effects section] The chance of CVD death unvaxed is 3000/ mill for a 60 yo, less than 20/ mill for a 26yo, and less than 2/ mill for those under 18yo.
[Long Covid chance < 50-80/ mill child to 230/mill for an older adult]
Additionally, slide – C4 below provides another good presentation of the effectiveness of vaccines in reducing the chance of death.
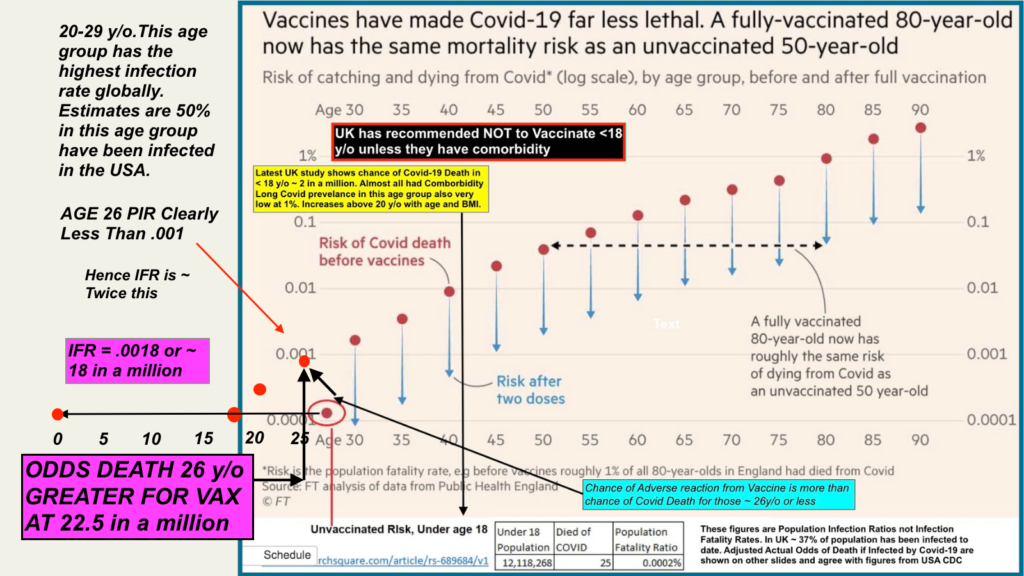
Slide – C4 – Vaccines Have Made Covid-19 Far Less Lethal
Firstly -The Conclusions, Followed By Explanations.
To Vax Or Not To Vax – Conclusions:
If you are over 65 – GET VAXED YESTERDAY!
If you are above 35, GET VAXED.
If you are ANY AGE and have serious comorbidity – GET VAXED! That includes obesity or very high BMI, heart disease, diabetes, lung disease, managing cancer etc. [*People of Colour, Hispanics, and South Asians also appear to be more at risk of Severe Disease and should consider themselves in this group]
If you are between 26 and 35 and healthy – GET VAXED if you are concerned about Long Covid.[ LC < 50-80/ mill child to 230/mill for an older adult see LONG COVID section] Otherwise, DON’T depending on personal circumstances. If you are not concerned about Long Covid the primary reason to get vaccinated is to stop spreading the disease. You are in MORE danger of FLU death than COVID death. You are the people with real choice. Given the latest developments with breakthrough infections and transmission, in my view, DON’T, subject to personal circumstances. (Regular Interaction with the very vulnerable as a deciding factor.)
IF You are HEALTHY and under 26 – DONT GET VAXED. Vax Risk is > Covid Risk. Vaxed Can Get And Easily Spread Now. [Read HERE for a peer-reviewed article written in 2018 – pre CVD – warning of the dangers of mass vaxing those not at risk.]
Children should not be vaccinated. (As per UK government advice)
This post is a GUIDE ONLY specifically in relation to AGE. You should SEEK PROFESSIONAL ADVICE in relation to your own health circumstances and vaccine suitability.
Unlikely – But Just In Case *UF* CONCLUSIONS:
SLIGHTLY WORRIED ABOUT VAX (UF)*
If you partly believe the UF* arguments and those of the Professors mentioned in the ADVERSE EFFECTS sections and are slightly worried about the vax
- ABOVE 45 consider vax,
- BELOW 45 don’t get vaxed. Below 45 there is no greater chance of death from CVD than regular flu.
2. EXTREMELY WORRIED ABOUT VAX SAFETY AND ADE: (UF)*
If you are extremely worried and believe ADE is starting to occur (in the Pfizer vax moreso is a possibility) or that the mRNA vaccines may have long term effects as yet unknown:
- If you have access to new treatments such as monoclonal antibodies – Don’t get vaxed.
If no access to such treatment:
- ABOVE 65 consider other than an mRNA vax such as AstraZeneca
- BELOW 65 unless unhealthy with comorbidity, Don’t get vaxed.
Above 65 the odds of CVD death increase dramatically. Delta is extremely contagious so its increasingly likely in time most people will be exposed. It may well be less deadly after a few years – right now thats not the case.
Explanations
Effectiveness of the Vaccines is proven
THE VACCINES WORK (For ~ 6 months)
Pretty straightforward. The chance of death is enormous for some, and data from all over the world clearly shows the vaccines we are talking about in this post are working in preventing severe disease and death in the most vulnerable – the very old and/or unhealthy. Benefits outweigh any risk by a country mile for that group. [Note (UF)* claims oppose this view.]
See UK data and graphs below showing how effective vaccines are in the UK population.
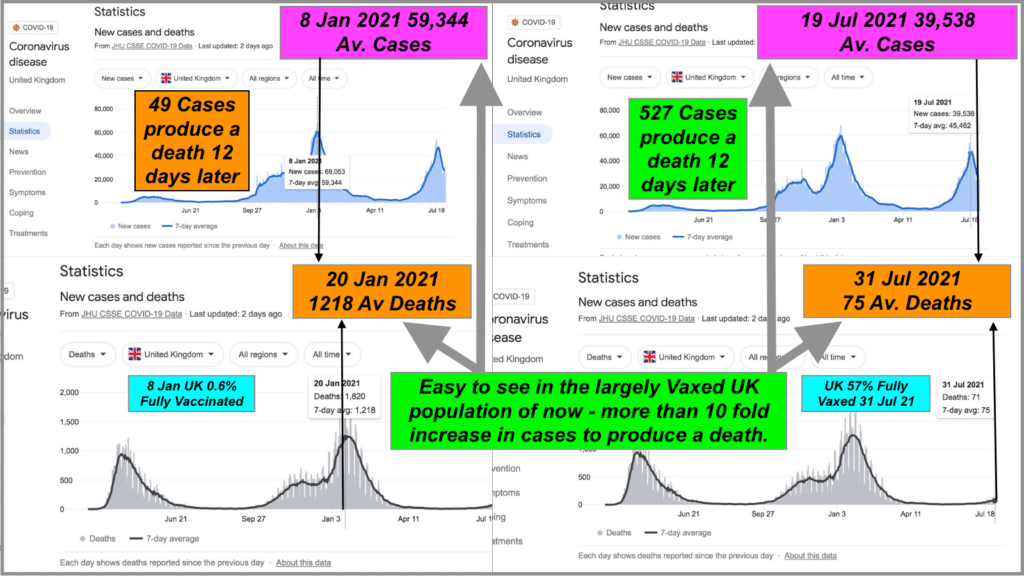
Slide C5 -Vaccines Work In UK
Vaccination rate of 57% on 31 July 2021 shows a 10 fold reduction in cases to death ratio since Jan 2021 when just 0.6% population was vaccinated. [Ref :New cases and deaths From JHU CSSE COVID-19 Data ]
Probable That Herd Immunity From Vax No Longer Relevant With Delta
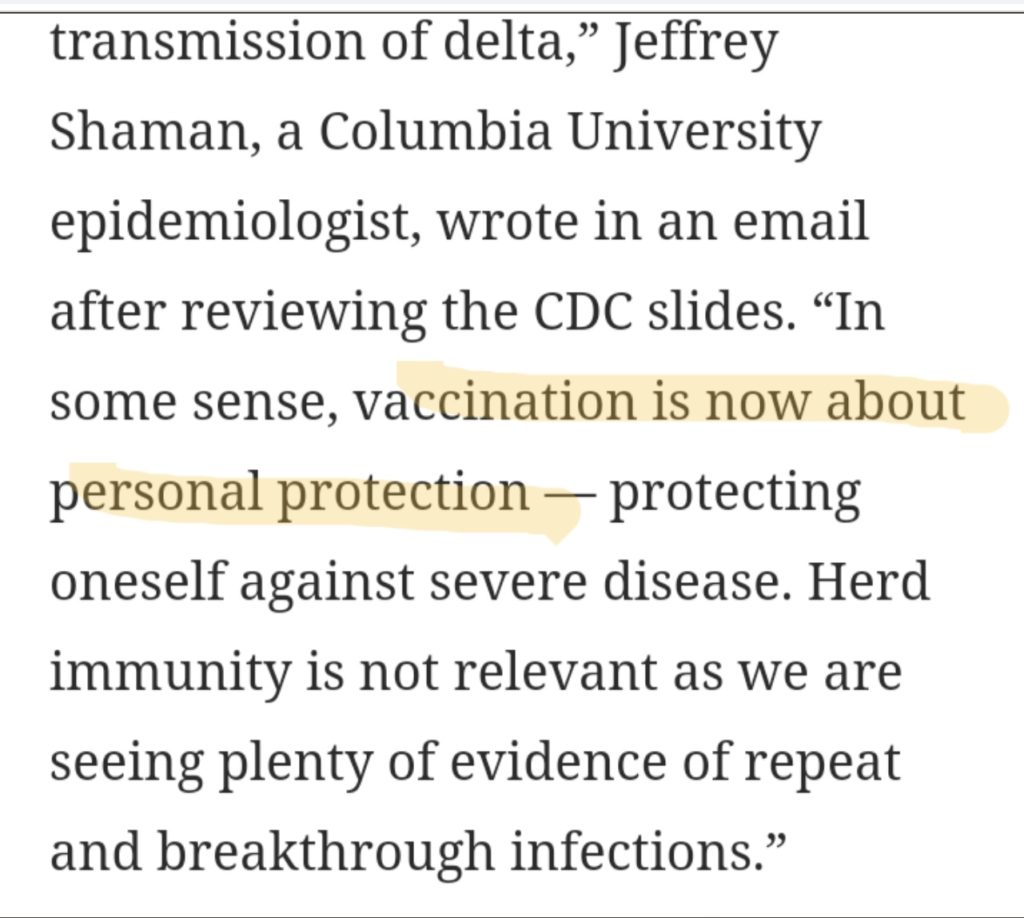
Vaccination is now about personal protection. Stopping the spread is no longer valid according to an increasing number of epidemiologists.
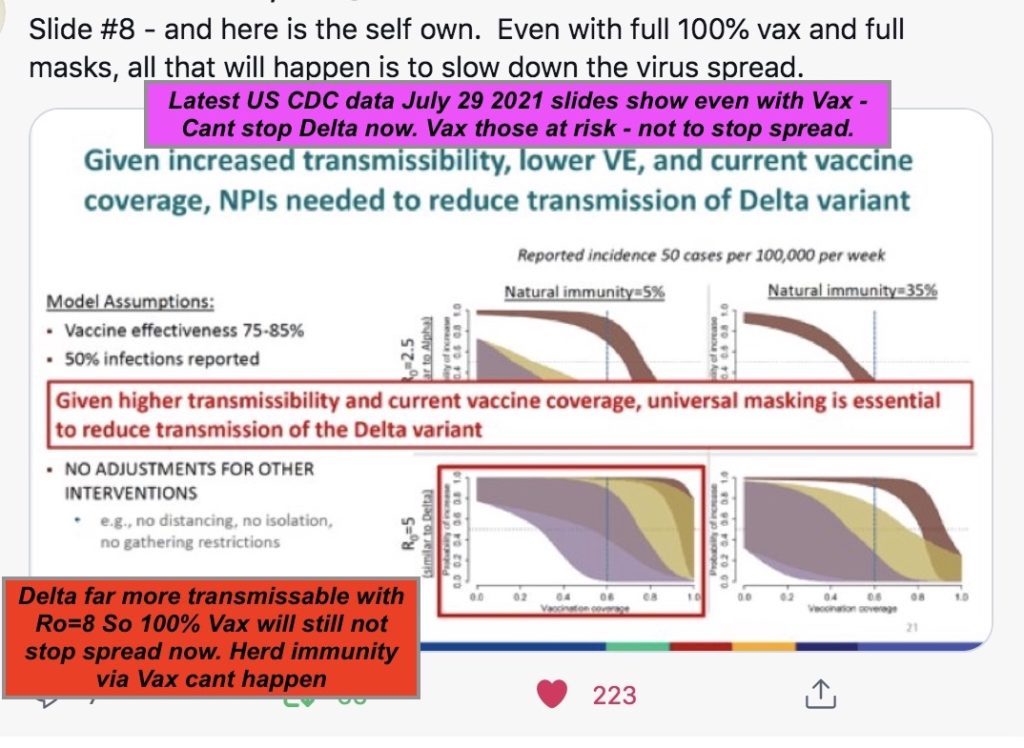
The latest US CDC Slides suggest that even with 100% vaxed, Delta will still spread. Herd immunity is not possible from these Vax.
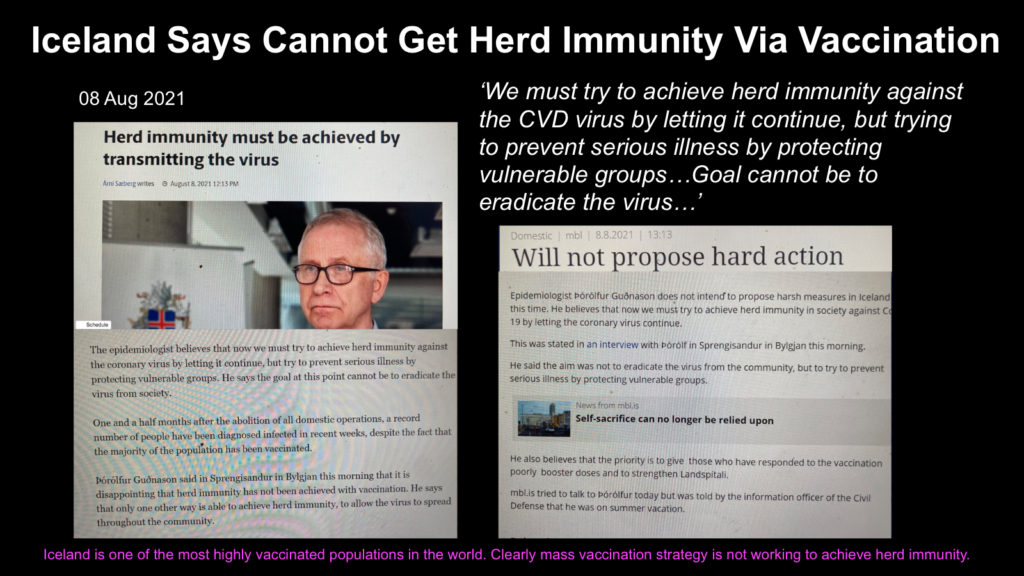
Iceland has over 86% of its population vaxed. Delta is running rife – so far not excessive death but plenty of hospitalization. Herd immunity via vax alone seems impossible. A strong argument for natural immunity in the young/healthy – after a usually mild infection – is mounting.
Long Covid
Symptoms of Long Covid
The ten most commonly reported symptoms in Long CVD (LC no. of days it lasts) are fatigue, shortness of breath, muscle pain, cough, headache, joint pain, chest pain, an altered sense of smell, diarrhea, and altered taste.
Other common symptoms include ‘brain fog’ – when thinking is fuzzy and sluggish – memory loss, disordered sleep, heart palpitations, and a sore throat.
The condition is not life-threatening, however, in some rare cases, it can persist and affect quality of life. Serious Long Covid (LC) is an extremely rare outcome where debilitating symptoms last for longer than 8 months. See article here about Long CVD from the University of New South Wales.
Vax will help prevent Long CVD – largely proportionately to the chances of severe outcomes of CVD. Latest studies show LC56 – LC84 may only be prevalent in ~ 1 to 1.6% of those under 18.
Children and Long Covid
A UK Royal College of Paediatrics and Child Health expert said the data reflected what doctors saw in clinics;
- Compared to adults, children are far less at risk of coronavirus.
- Many who are infected do not develop symptoms and those that do, tend to have a mild illness
- Long-lasting Covid-19 symptoms are very rare in those under 18.
The largest and most recent peer-reviewed study confirming this – including data from ‘Delta’ variant – was published in the Lancet Child and Adolescent Health journal in August 2021.
Chances Of Long Covid With Age
The chance of Long Covid – where some symptoms persist for more than 12 weeks (LC84) – for adults has been found to be around 2.3% now for those who contract CVD.[May2021]
[13.3% ≥ 28 days LC28, 4.5% for ≥ 8 weeks LC56 and 2.3% for ≥12 weeks LC84]
It is NOT an issue for children, as the largest most recent study published in the Lancet 03 Aug 2021 has found at less than 1.8%
[4·4% for LC28 ,1·8% for LC56 and less 1.6%LC84]
A recent study (yet to be peer-reviewed) found 80% recover completely within 8 months. That implies 20% of these adults [LC84 2.3%] or around 4600/ mill may continue to exhibit symptoms, although, in the vast majority, these are not debilitating. Assuming the worst case of ~ 5% for extreme & lasting debilitating symptoms, would mean around 230/ mill of severe sufferers (older) may have Serious Long Covid (LC). [Vax adverse effect (27.5* *Add 18/ mill to account for Pericarditis -121/ mill)]
The vaccines can help prevent serious Long Covid (LC) for older adults
For children, there is little evidence of LC84. Even 1 -1.6% prevalence would imply a < 50 – 80/ mill chance of serious LC.
Importantly the study found for children the most common lingering symptoms were mild with:
- tiredness 3%
- difficulty concentrating 2% and
- increased need for sleep 2%
Given the seriousness of the adverse effects due vaccines of DEATH, paralysis or long term heart complications at (27.5 -121 /mill):
The vaccines are more dangerous to children and those under 26 yo than the risk of Long Covid (LC84) or LC
LC appears to be worse in those with severe disease but can affect those with mild symptoms.
For those 26 to 35 yo the risk of severe disease increases slightly so therefore the risk of LC also increases. A 35yo has 120/ mill chance of death due CVD. This is now similar to the chance of serious adverse outcome from the vaccine and also the chance of serious LC. [LC < 50-80/ mill child to 230/mill for an older adult]
LC is more of an issue for those over 35 yo and the vaccines can help prevent LC
The majority of sufferers are in their mid to late 40’s, with most severe symptoms occurring in those who had the most severe disease. Being older, female, and hospitalized at symptom onset were found to be significantly associated with an increased risk of developing LC84 & serious LC.
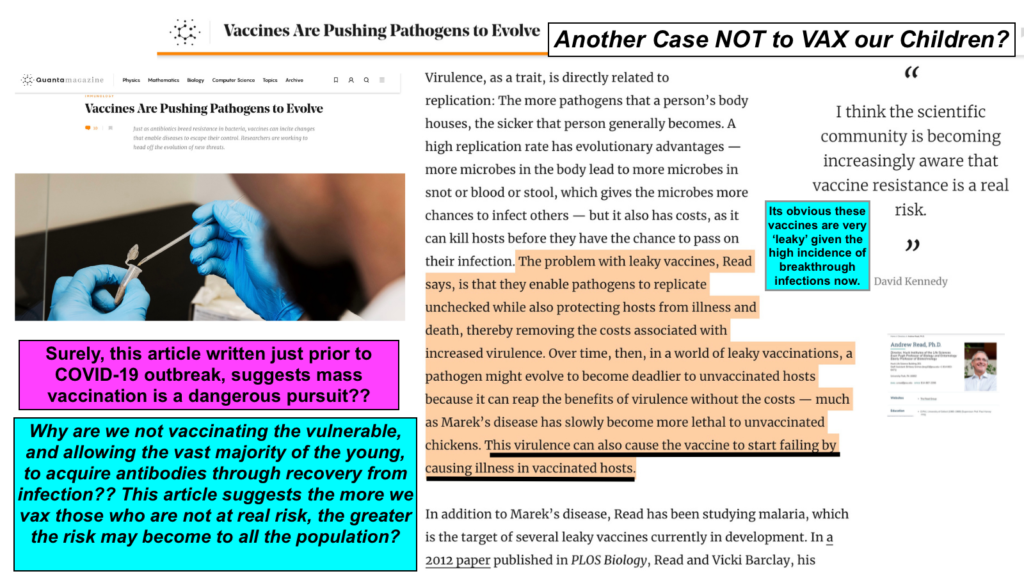
The Risk Of Leaky Vaccines
The current vaccines ARE ‘LEAKY’. They stop infection by as little as [University College of London] 23.7% and once infected, Delta variant spreads easily in the vaccinated. There are many studies showing the potential problems with leaky vaccines. An important one:
‘Imperfect Vaccination Can Enhance the Transmission of Highly Virulent Pathogens’
may give some reasons as to why more CVD strains are evolving. Another as shown below provides similar conclusions.
ADE – Antibody Dependent Enhancement (UF)*
ADE – (UF)*an extremely dangerous outcome where the vaccine can fail and increase the severity of the virus in those vaccinated
This happened previously with attempted vaccines for Coronaviruses, HIV, Measles, Dengue Fever, and others. Up until the ‘Delta’ strain and as recently as 29 Jun 2021 – this was thought of as extremely unlikely. New contrary modeling evidence in the ‘Journal Of Infection’ – yet to be peer-reviewed – has been documented on 9 Aug 21 and is shown below. (UF)* This disastrous outcome still appears very unlikely to eventuate. If it did, however, it could potentially mean new booster rejigged ‘vaccines for the vaccines’ may have to be administered.(UF)*
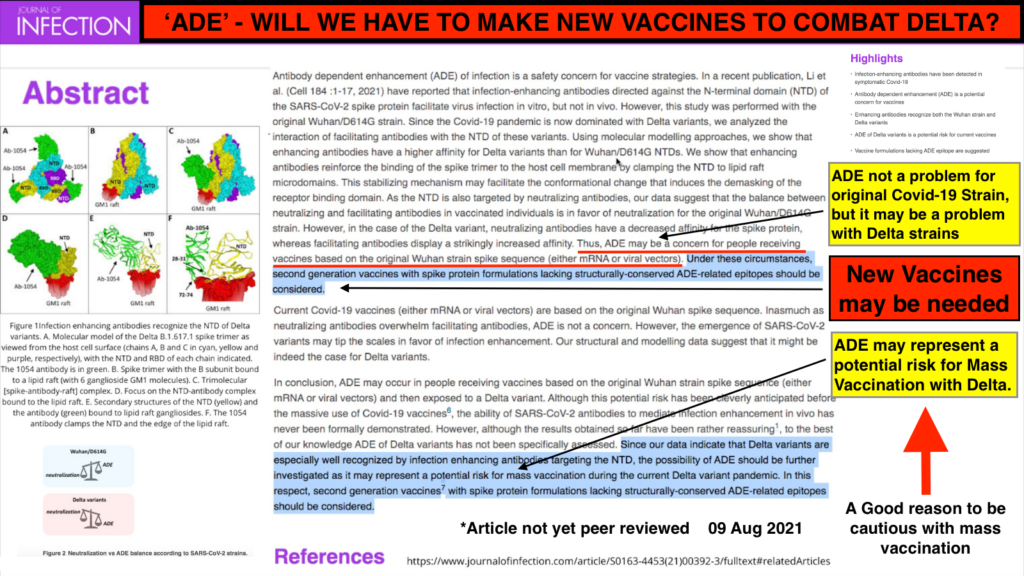
ADE may still be an issue with Delta. (UF)* August 09, 2021 Read here
Natural Immunity From Infection Recovery Is Likely Better Than VAX
There are numerous studies regarding convalescent immunity in recovered CVD patients. Conclusions from the latest ( yet to be peer-reviewed ) study show that
Natural immunity confers longer-lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity.
The EU and many countries recognize recovery from CVD as a condition for their vaccine passport for a period of 6 months. Yet another recent study – to be peer-reviewed – suggests ‘ that broad and effective immunity may persist long-term in recovered COVID-19 patients.’
‘Exposure and recovery will give better immunity than vax’ according to the latest real-world practical results study from Israel. Coronavirus patients who recovered from the virus were far less likely to become infected during the latest wave of the pandemic than people who were vaccinated against COVID, according to numbers presented to the Israeli Health Ministry.
Nearly 40% of new COVID patients were vaccinated – compared to just 1% who had been infected previously.
US CDC Covid-19 Death Data Was Not Scrutinised For Child Comorbidity [READ HERE]
It is very clear that comorbidity (including ethnic origin) at any age has a huge impact on CVD outcomes.

It Appears Governments Of The World Are Simply Copying The USA In Approving Child Vaccination.
A Stronger Argument Now Exists To Vax The Vulnerable Only
Given the latest developments in highly vaxed countries, the possible leaky vaccine outcomes, and even the remote possibility of ADE *(UF) [See Adverse Effects] with Delta, the argument to change strategy & vax the only the vulnerable is gaining more attention.
Clearly, the vaccines are not producing herd immunity as was hoped in the mass vax strategies adopted by Israel, Iceland, and other countries. Hospitals are seeing record cases of transmission and admissions of the fully vaxed.
An article 05 Aug21 in the Washington Times can be read here explaining how:
‘the mass vax strategy will now most likely prolong the most dangerous phase of the pandemic’
‘A far more optimal strategy is to vaccinate only the most vulnerable. This will limit the amount of vaccine-resistant mutations and thereby slow, if not halt, the current vaccine arms race.
Fortunately, those most vulnerable represent a relatively small number; and these cohorts have already achieved high levels of vaccine acceptance. They include senior citizens, for whom the risk of serious disease or death increases exponentially with age, and those with significant comorbidities such as obesity, lung, and heart disease.’
The article is co-written by Dr. Malone – a controversial* pro-vaxer & co-founder of mRNA technology. *His views are pro-Vax – but he disagrees with the rapid release to the public of the CVD vaccines. (He suggests ADE studies were overlooked for example.) In this article, his arguments align with those of Prof. Read in the “Leaky Vaccines” peer-reviewed article presented previously. [See Adverse Effects *(UF) Dr Malone]
A Focussed approach – Great Barrington Declaration
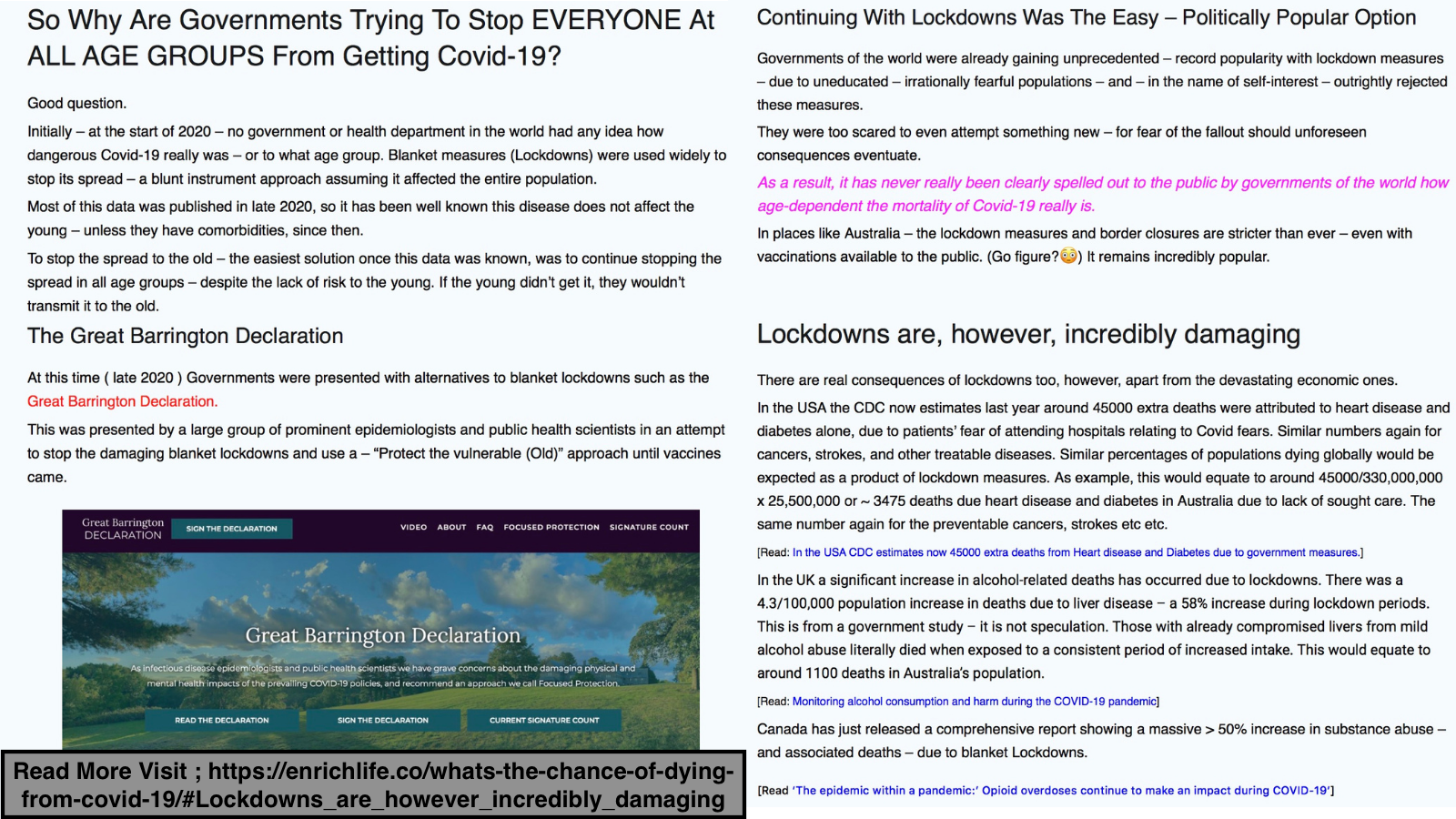
In late 2020, The Great Barrington Declaration was presented by a large group of prominent epidemiologists and public health scientists in an attempt to stop the damaging blanket lockdowns and use a – “Protect the vulnerable (Old)” approach until vaccines or treatments came. This was largely discredited at the time, for lack of detail and what appeared to be risky assumptions. With vaccines available now, however, this would seem to be a valid solution. Rapid antigen tests could be used to help protect the vulnerable who cannot be vaxed until herd immunity – or as close as possible to it – was achieved. New treatments such as monoclonal antibody treatment as approved on 02Aug21 in the US can now help.
Currently, globally governments are enjoying record popularity with blanket lockdown measures, but the latest developments may force their hands into change. The WHO is already calling for vax to be sent to the vulnerable worldwide and not given as booster shots to those with little risk.
Regardless it makes little sense now to vax those who are not at risk from CVD.
ADVERSE EFFECTS DUE TO VACCINATION
There are definitely risks with all vaccinations and the Covid-19 Vax’s are no exception. They are extremely rare, but real nonetheless.
The published – acknowledged severe risks of the vaccines researched in this post are:
27.5**Add 18/ mill to account for Pericarditis to 61.5/ Mill – up to 121/ Mill
To compare, the risk of Covi-19 death if infected is:
- under 18yo < 2/ Mill,
- 25 yo < 20/mill,
- 27 yo ~ 30/mill
- 30yo ~ 60/mill
- 35 120/mill, 40 200/mill, 45 1000/mill, 60 3000/mill,
- 80 50,000/mill, 95yo 200,000/mill. [See Slides C3/ C4]
- Age ~ 26 and below Vaccine risk is greater than Covid-19 risk.
Vax risk includes death, and severe outcomes such as anaphylaxis, TTS – (blot clots) thrombosis with thrombocytopenia syndrome, cardiac disorders such as myocarditis (inflamed heart), Guillain-Barre syndrome (GBS), and more.
Research shows acknowledged risks as published in gov. data from:
- TGA Australia,
- CDC USA,
- The European Centre for Disease Prevention and Control (ECDC),
- and the Canadian Govt.
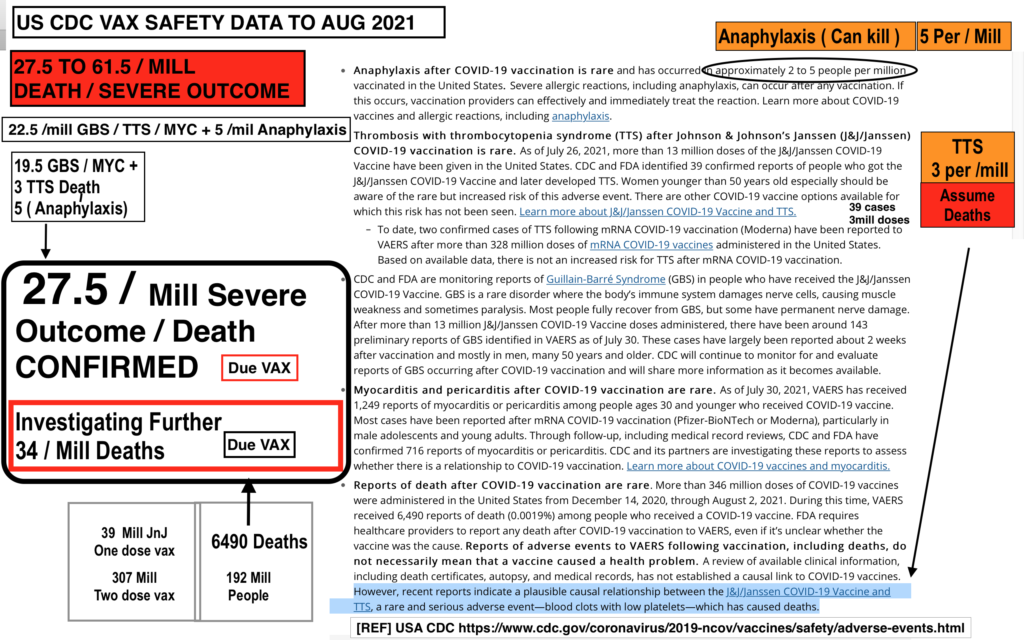
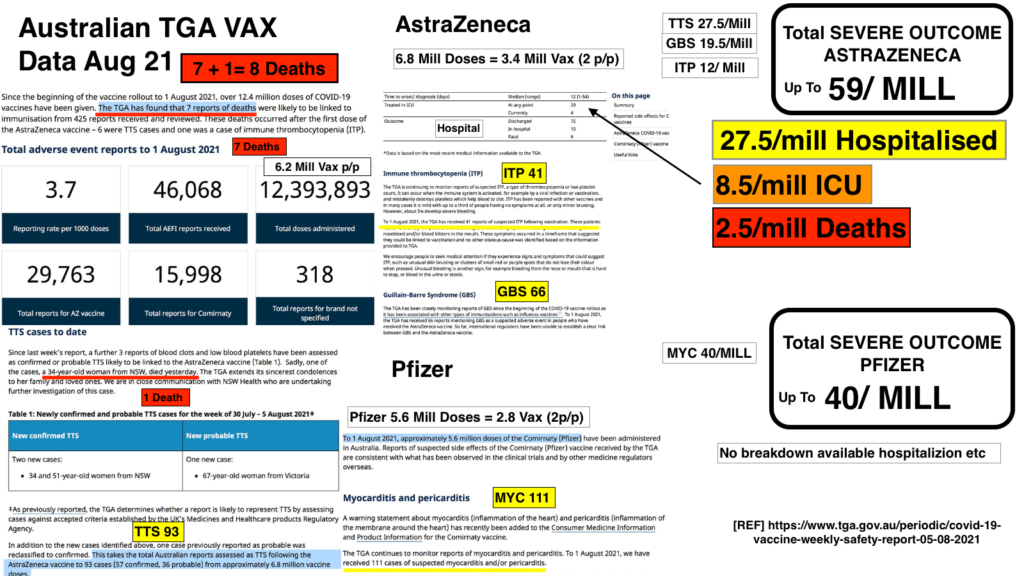
For example, TGA Australia found ~ 2.5/ mill chance of deadly blood clots for AstraZeneca, and USA CDC found ~ 3/ mill chance for all vax. TGA Australia found ~ 19.5/ mill chance of GBS in Astrazeneca, CDC found 7.5/ mill, and all agencies found ~ 5/ mill chance of anaphylaxis. CDC found ~ 22 -27/ mill myocarditis and pericarditis in < 30 yo males, and av. in all ages of ~ 10/ mill. Overall TGA found 27.5/ mill hospitalizations with 8.5/ mill needing ICU.
[See slides A1 to A4 below ]
The greatest volume of vax data available is from US CDC:
Severe Vax Risk is (27.5*Add 18/ mill to account for Pericarditis to 61.5*/ Mill) [CDC 10 Aug 2021]
*CDC investigating a further 34 /mill deaths. [See Chart A1]
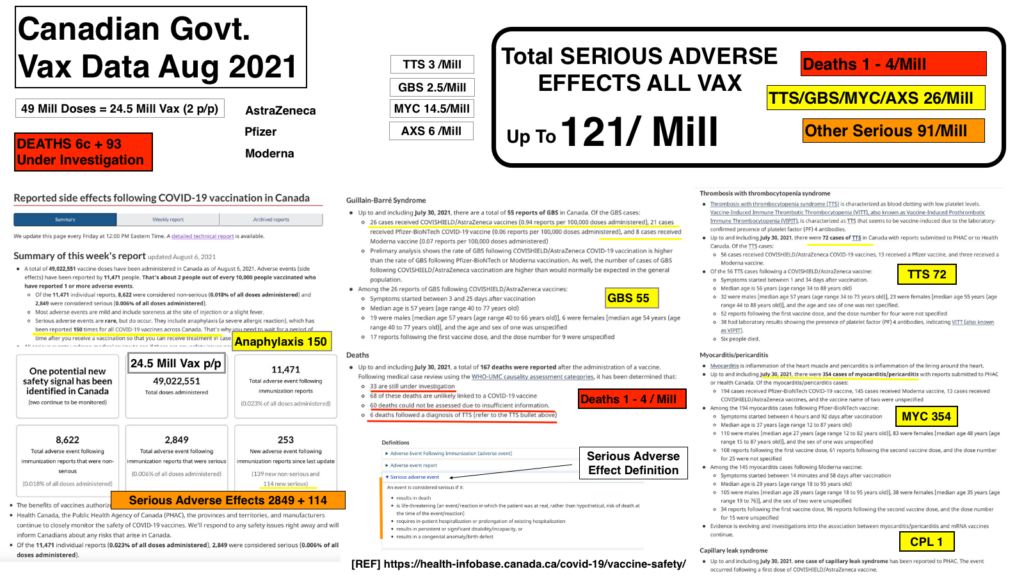
All govt data shows a minimum of 27.5/ mill severe risk. Canadian Govt data shows vax risk could be up to 121/ mill [See slide A4] & Europe/ UK are investigating up to 102/ mill deaths in the fully vaxed. [See slide A5]
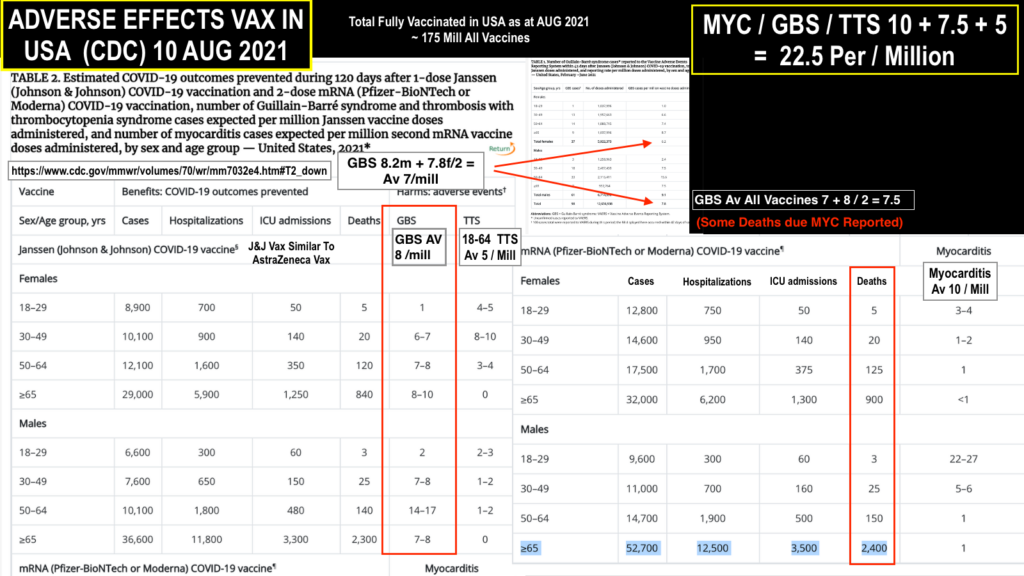
Slide A1 [REF US CDC HERE] *Add 18/ mill to account for Pericarditis
Slide A2 – Shows CDC acknowledged
Chance of Severe Outcome Due To VAX is Between 27.5* – 61.5 Per/ Mill *Add 18/ mill to account for Pericarditis
(Chance of Death due CVD same as 26yo to 30yo)
27.5* /mill *Add 18/ mill to account for Pericarditis are the odds of
A SEVERE – LIFE THREATENING reaction to the vaccine.
This is greater than the odds a 26 yo has of a severe Covid-19 outcome if infected.(See slide C3)
Confirmed – Published Data Shows AGE 26y/o & Lower Have A HIGHER RISK Of SEVERE OUTCOME From The Vaccine Than From Covid-19 Infection. [REF US CDC 10 Aug 2021]
Why get vaxed if there is no benefit to oneself, JUST RISK?
For every 36,000 vaccinated, one may die from the vax. If seven million (e.g Australias under 26 population) were vaxed ~ 193 deaths would be expected due vax, 151 MORE than the ~ 42 deaths due to CVD. (Av. 6/mill chance of death CVD all < 26 yo’s) [See slides C3/C4]
Slide A3 *Add 18/ mill to account for Pericarditis
Slide A4 *Add 18/ mill to account for Pericarditis
‘Unlikely but just in case’ figures. (UF)*
Mistrust Of Big Pharma (UF)*
One of the greatest causes of ‘NOT TO VAX’ is the mistrust of big Pharma companies such as Pfizer and the data they provide to confirm the vaccines are indeed totally safe. When such ENORMOUS sums of money are involved, this is totally understandable.
Pfizer was recently accused of “bribing doctors and suppressing adverse trial results.” Pfizer has settled various lawsuits that involve allegations of kickbacks, fraudulent marketing and data manipulation- the cost of settlement is unknown and no wrong doing admitted. $2.3 billion was the total amount of a settlement involving Pfizer in a separate lawsuit where Pfizer falsely promoted some of its products. The company had to pay approximately $1bn to Medicare, Medicaid, and other government insurance programmes under the settlement. [Ref FACTCHECKER]
There are also numerous well respected medical professionals involved with vaccine development – who publicly question the validity and scrutiny of the published data relating to vaccine trials. There is no question these vaccines have been produced and have (mostly ‘Emergency’) approval in record time. There is undoubtably enormous numbers of lives of the old and vulnerable already saved due to this. However, the lingering doubt still remains for many who are not in the high risk group, and feel they are being coerced into getting vaxed.
Mistrust Of US CDC (UF)*
Summary Of Reported Deaths and Adverse Effects HERE
There is no doubt that it is in human nature to often succumb to the influence of power and money. The following is from vocal opponents to the rapid vaccine approvals. For example, the following data comes directly from reports submitted to the USA CDC Vaccine Adverse Event Reporting System (VAERS).
It is not yet, and may never be, confirmed these
adverse effects were due specifically to the vax.*(UF)
Between Dec. 14, 2020, and June 11, 2021, a total of 358,379 total adverse events were reported to VAERS, including 6,340 deaths — an increase of 105 deaths over the previous week. There were 29,871 serious injury reports, up 1,430 compared with last week. Total vaccines given were 306.5 million.
It should be noted that CDC USA also has a history of some incorrect assessment of reporting.
Recently John Hopkins researchers found that ZERO of the CDC reported deaths under 17 y/o were in fact due to Covid-19, rather they were from comorbidity.
The chance of serious injury or death from the US VAERS data is 117/ mill & same as those for a 35 yo of a severe CVD outcome. See Slide C3. (Note Candian govt data has an upper limit of similar at 121/ mill.)
If these are confirmed, it means anyone 35 years old or lower has MORE CHANCE of VAX Death/ Serious injury than Covid-19 Death. *(UF)
For every 8,500 vaccinated, one may die. If 10.7 million (e.g Australias under 35y/o population) was vaxed ~ 1260 deaths would be expected, with no expected benefit.*(UF)
Latest Reported Adverse Effects From UK/ USA/ EUROPE (UF)*
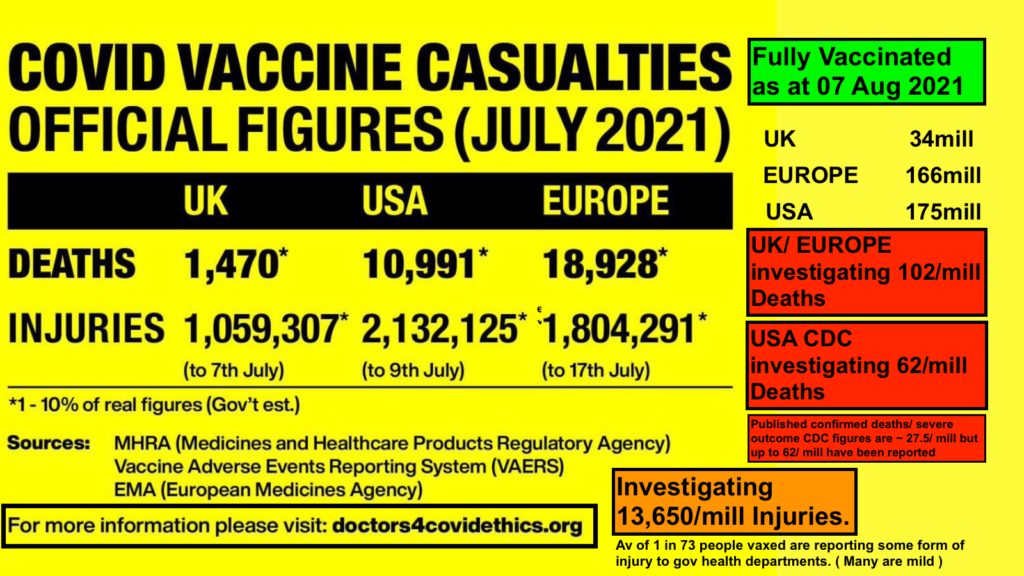
Slide A5
A group of doctors globally have formed doctors4covidethics.org and publish government health authorities’ data from the UK/EU/USA. These figures show the possibility of higher than the US VAERS 117/ mill, or CAD govt limit of 121/ mill chance of death or serious injury due to the vax (UF)*
Prominent Professors Opposing The Vax Regulatory Process & Safety Particularly For The Young (UF)*
A prominent opponent to the vaccine trial process, Dr. Peter McCullough is one of the most cited medical doctors on COVID-19 treatments at the National Library of Medicine, with more than 600 citations. He has testified before Congress and won numerous awards during his medical career. Dr Robert Malone, a co-inventor of mRNA vaccines as used in Pfizer and Moderna, and RNA as a drug, shares similar views with Dr McCullough.
Dr Malone worries due to insufficient trials there is still a chance vaccines may ultimately cause ADE as discussed previously in [Expalnations – Leaky Vaccines – ADE]
ADE – an extremely dangerous outcome where the vaccine can fail and increase the severity of the virus in those vaccinated*(UF)
The latest world data showing waning of the efficiency of the vaccine is the greatest danger period according to Dr. Malone.
A very new study also suggests it could be a problem with the CVD ‘Delta’ strain, and if so new vaccines would be needed.
Hopefully, the latest world events are NOT indicative of ADE. (UF)*
The evidence certainly suggests however there is no point in vaxing those not at risk of CVD ( Young/Heathy)
Click here to see the Israeli news reel
More Safety Concerns (UF)*
Dr. McCullough – whilst still agreeing vaccines have been life-saving for many vulnerable, suggests during US trials there was an understating of deaths and severe outcomes – and it should be acknowledged that vaccines caused 197 per million deaths.
He now claims that more like 50,000 deaths have been reported to USA CDC but covered up, and that evidence may suggest the vax are unsafe long term. He also wants the vax program to stop immediately, and he says the use of modern treatment methods such as monoclonal antibody treatment – which he largely pioneered – can manage the pandemic successfully when administered early after infection.
On Aug 02, 2021: FDA authorized monoclonal antibody treatment as preventive after exposure to Covid-19. In a recent interview on June 22 2021,
Read:
Dr. McCullough urged health authorities to stop administering
vax to under 30-year-olds due to the vaccine risks.*(UF)
See Video:
Dr. Peter McCullough – URGENT WARNING About Poisonous Jabs – “An Agonizing Situation” *(UF)
Dr. McCullough’s claims of > 50,000 deaths would mean > 260/ mill due to vax.
That would equate to any less than 40 yo having a greater chance of adverse effects due to the vaccine than due to CVD. *(UF)
In this scenario,10.7 mill < 35 y/o such as in Australia would lead to ~ 2700 deaths due to vaccination.(UF)*
Vaccine Passports.
Due to the Latest World Data it is firmly expected the current plans for vax passports will have to change. Currently, Europe allows privileges to those who:
- Have been fully vaxed or
- Can show proof of a blood test within 6 months showing recovery from CVD infection or
- Have a Rapid antigen test or recent PCR test confirming CVD negative.
In Latest World Data Delta variant has very recently been found to be far more contagious, and
- Vax is now far less effective against it in spreading the disease, – even vaxed can spread it easily.
- Vax efficiency has been found to wain considerably after 4-6 months to a point where it’s less than 39% effective at stopping infection ( Latest <8% Aug 21)
Quantitative Antibodies Test
Speculation is now that the Vax passport will have to require showing proof of a
- Quantitative antibodies test within 6 months or
- A recent PCR test or
- Rapid Antigen test before entry.
Natural immunity after recovery or a recent vax should provide the means to pass the quantitative antibody test. Simply being fully vaxed is now insufficient to prevent infection or transmission, so it is likely to become redundant as a lone condition in the vax passport. This also means the primary reason for the (very fit) young to get vaxed is now obsolete.
.

Latest world data shows Vax passports will have to change from the current form because vaxed can far more easily contract and spread D now…
Conclusions Further Explained
1). If You Are Over 65 – Get Vaxed Yesterday
No more discussion is needed.
2). If You Are Over 35 – Get Vaccinated
Above ~ 35 yo, the benefit of Vaccination outweighs the risk to the individual.
At age ~ 45 the risk of flu death is around the same as the risk of CVD death. See slide C3. These figures are approximations, so using age 35 is conservative and accounts for Long Covid and more chance of hospitalization above ~ 40 yo.
An unvaxed person < 35 has more chance of Flu death than severe outcome or death from Covid-19.
We don’t change our lives based on flu death chances and we generally don’t fear the flu.
Vaccination will also prevent Long Covid which is most prevalent in ~ 45 yo’s.
3). Comorbidity – Get Vaxed.
Overwhelming evidence from all over the world suggests CVD is more likely to have an unfavorable outcome in those who are unhealthy. This is true for ALL AGE GROUPS. In the latest UK study on childhood CVD, 25 children died with CVD from several million infections. Only 6 of these children were free of comorbidity. 56% of those who died were of Black or Asian ethnicity.
[Without comorbidity ( & including race risk ) UK figures show IFR of (ZERO < 1/ mill ) from this data.]
Obesity/High BMI, Diabetes, Heart, Kidney, Lung diseases, Dementia and neurological conditions, High Blood Pressure, Liver disease, the Immunocompromised all lead to a greater risk of severe illness unvaxed. It appears mild asthmatics may not be at increased risk due to the nebulizer effect. See here for a more detailed list from CDC USA.
People of Colour, Hispanics, and South Asians also appear to be more at risk of Severe Disease and should consider themselves in this group.
The rewards of vax – and chance to prevent CVD – outweigh the risk at every age.
4). Between 26 And 35 & Healthy – GET VAXED If You Are Concerned About Long Covid. Otherwise – Personal Choice ‘To Vax or Not To Vax.’
Personally – If healthy, I would NOT get Vaxed in this age group.
This is the most difficult group to make an informed decision regarding To Vax or Not To Vax. The chance of severe CVD and death is far less than that of the Flu, and the chances are high that CVD will not even seriously affect you. Hence Long Covid is possible [ 20/mill for serious long term] – but unlikely.
At 35 yo with CVD death odds of 120/ mill (1 in 8,500) – remember that means in large populations there will be some deaths reported. The CHANCES remain incredibly low for you as an individual. Remember also, the chance of death due to ALL OTHER CAUSES in this age group is 1650/ mill (1 in 600*) – FAR HIGHER than that of CVD. *[REF USA CDC]
I’ve had CVD – and I’m well above this age group. I was tired for two days and lost my smell for two weeks. That’s it. Everyone is different of course.
The relevance of the (UF)* figures in terms of vaccine safety comes into play in this age group. If you believe Big Pharma has covered up results, or that the outspoken doctors as mentioned in the ADVERSE EFFECTS section are correct, then dont get vaxed.
The Primary Reasons FOR VAX Between 26 & 35.
To Stop The Spread To The Vulnerable (Largely NOT APPLICABLE given latest world data regarding the fact vaxed can get AND spread Delta.)
To Prevent Long Covid. (See Long Covid section)
Vaccine Passports. – Most likely plans for these will need revision due to the latest world data and Delta. (See Vax Passport)
The Primary Reasons NOT TO VAX Between 26 & 35
Covid Is Increasingly LESS Deadly Than The Flu With Youth. – it’s simply not a dangerous disease for the vast majority.
Latest World Data Shows Vaxed Can Increasingly Get And Easily Spread Delta
Recovery From CVD Now Shown To Give Better Immunity Than Vax.
Adverse Effects Due To Vaccination. Published vax Death/ Severe Odds are (27.5 – 61.5/ mill) up to 121/ mill. That means those under (26 – 35 yo) have a greater chance of Death due to vax than Death due to CVD. See Slide C3
Chance Of ADE or Other Unknown Vax Long Term Harm.
5). IF You Are HEALTHY & Under 26 – DONT GET VAXED. Vax Risk Is > Covid-19 Risk. Vaxed Can Get And Easily Spread Now.
The reasons have already been explained for this in previous sections. There is no advantage now for any healthy under ~ 26 yo to get vaxed.
The chance of a severe outcome from CVD (2 – 18/ mill) – is LESS than
the chance of a severe outcome from the vax! (27.5* *Add 18/ mill to account for Pericarditis – 121/mill)
Additionally:
- Under 26 yo risk from Covid-19 borders on extremely low to negligible. [Slide C3/C4]
- Delta spreads and transmits regardless of vaccination so being vaxed will not ensure the protection of others. [See Latest World Data]
- Natural immunity from a mild (or likely asymptomatic) infection is likely stronger, more diverse, lasts longer, & will more quickly result in herd immunity.
- There are real dangers to unnecessary mass vaccination with leaky vaccines.
- There is a definite – (possibly seriously understated)*(UF) risk with vax, but no benefit unless unhealthy.
- In the USA (no doubt soon elsewhere), monoclonal antibody treatment is now available to those testing positive. Other treatments are in trials.
- The long-term risks of the vaccines are unknown so surely it is better to wait until they are known
- Vaccines require booster shots every 6 months with the added risk of severe adverse effects.
- The chance of death at this age of all other causes is 500/ mill ( Borderline irrational to fear CVD this age.)
Recent article suggesting Delta COVID-19 variant could put younger people at risk of deadly cardiac complications
A recent article HERE suggests there is anecdotal evidence of up to a 450/ mill chance of myocarditis presenting in the young ( 12 – 17 y/o ) with Delta. The study is not peer-reviewed and involves 14000 living survivors of covid-19. Published data says vax causes 27.5 actual deaths or severe life-threatening illness/ mill & anecdotal evidence from CDC suggests a further 34 /mill actual deaths have occurred with the same disease due to vax. Anecdotally up to a further 260/mill actual deaths occurred from other vax complications.
The real-world facts are to date, in the UK’s population of 68 million, less than 2 in a million children under 18 have actually died due to covid-19 and in the USA, ZERO under 17 yo in a population of 330,000,000.
The Mathematics Of Very Large Numbers
What must also be remembered, is that the mathematics of large numbers will produce visible numbers of people in this age group becoming sick from CVD, and possible deaths. See ADVERSE EFFECTS DUE VAX section. The fact that ‘D’ is way more infectious- as much as chickenpox – means increasingly more young people are being found with the virus in most populations. To date it is not found to be more deadly. Risk for CVD infection is greatest in the 18-29 age group globally.
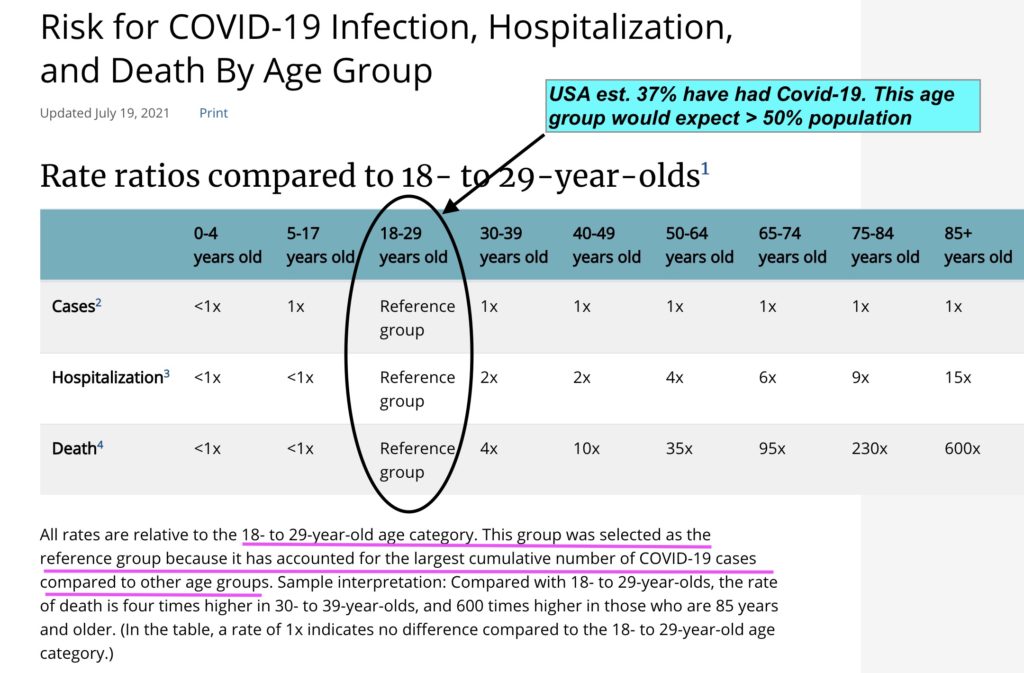
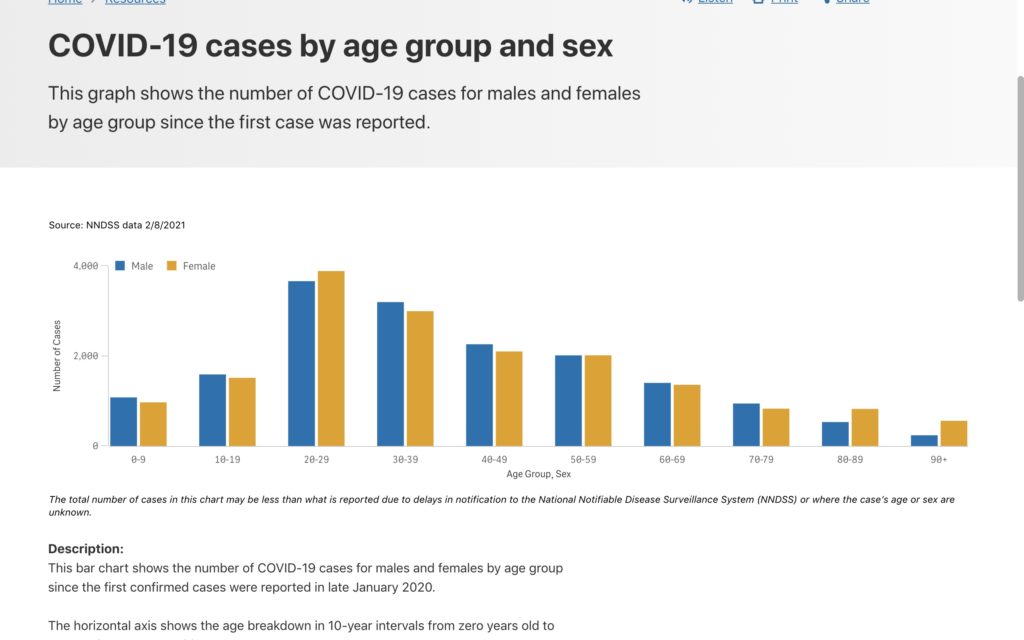
Risk for CVD infection is greatest in the 18-29 age group globally, but deaths and hospitalisations are not proportionate
The fact the older are mostly vaxed now adds to the proportion of cases in this age group. Deaths and hospitalizations are not proportionate, but media and governments with agendas love these events and tend to focus on them unfairly in some instances.
The point is, from published and acknowledged govt. data, there is likely to be MORE numbers of the dead or seriously ill due to getting vaxed in this age group than from CVD.
It seems policy in some countries (eg Australia), has not caught up with the latest world data. Previously the idea of reducing virus spread to obtain herd immunity if vaxed was logical for the benefit of the overall population (albeit unwise individually.)
Now there is simply NO GOOD REASON for very fit under 26 yo’s to get vaxed.
- The vaxed get infected and transmit.
- Herd immunity via vax seems impossible with Delta, even if 100% vax rate was achievable.
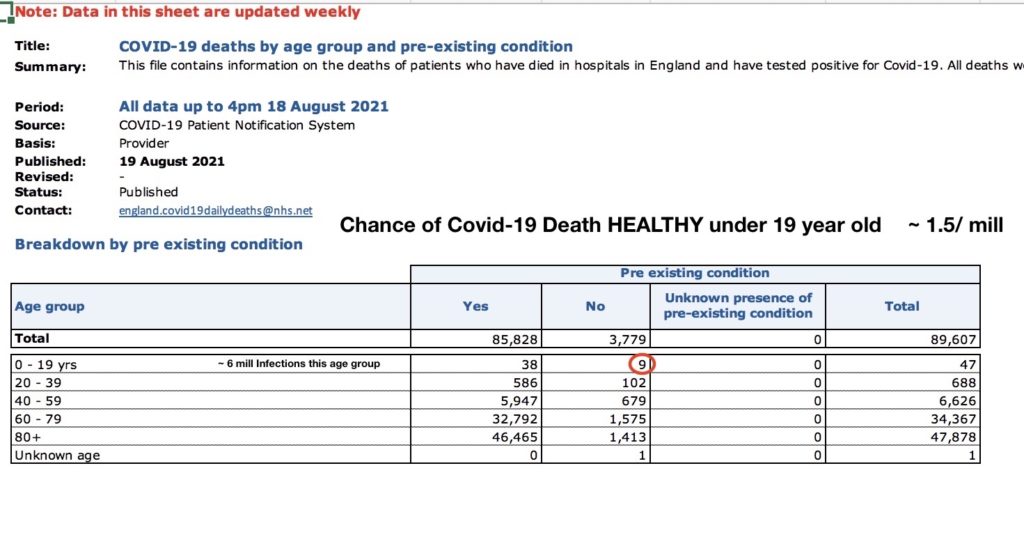
UK data shows less than 1.5/ mill chance of HEALTHY children at risk of Covid-19. The vaccine adverse effect risk is greater than this
Australian data supports the fact CVD is an old/ unhealthy persons disease. More than 57% of infections have been in the under 40 year olds with 0.4% of total deaths, and ZERO deaths in those under 20 yo.
6). Children Should Not Be Vaccinated. (As Per UK Government Advice)
Clearly since vaxing those under 26 is not logical then vaxing those under 18 makes even less sense. All world data shows the danger of CVD reduces significantly with age.
The chance of a severe outcome from the vax (27.5* *Add 18/ mill to account for Pericarditis – 121/mill) is MORE than:
the chance of a severe outcome from CVD (< 2/ mill)
Additionally:
- Healthy children’s risk from Covid-19 borders on negligible.
- Delta spreads and transmits regardless of vaccination.
- Natural immunity from a mild (or likely asymptomatic) infection is likely stronger, more diverse, lasts longer, & will more quickly result in herd immunity.
- Children are less infectious than adults naturally,
- There are real dangers to unnecessary mass vaccination.
- The long-term risks of the vaccines are unknown so surely it is better to wait until they are known.
- Vaccines require booster shots every 6 months with the added risk of severe adverse effects
- The chance of death at this age of all other causes is 500/ mill ( Irrational to fear CVD this age.)
Before the latest world data came to light, Professor Adam Finn, a member of the UK government’s JCVI, says ‘We cannot vaccinate children simply for the benefit of adults’. Professor Finn is an epidemiologist and pediatrics expert at Bristol University. He concluded: There is not enough evidence to justify vaccinating children against COVID as they are “less infectious than adults” and their risk from the virus is “vanishingly low.”
The latest world data now shows there is little or no benefit to the population due to ‘Deltas’ ability to compromise, infect and spread amongst the vaccinated. Read here – as of late July 2021 data shows only real benefit to vax now is stopping severe disease in the vulnerable. (Old/unhealthy)
THERE IS NO BENEFIT – ONLY RISK – TO VAX HEALTHY CHILDREN
They have suffered enough is so many ways already due CVD measures taken
We Need To Be Rational


We need to be rational. Assess the risk and respond accordingly with logic. Irrational Fear does nothing to help.
I’ve had Covid-19 as have several middle aged friends. I was tired for 2 days and lost my smell for 10 days. 85% of Vietnam’s population have been asymptomatic – they didn’t know they had it until tested. It can be dangerous – but is NOT a certain-death sentence. Do the research regarding your own odds – but PERSPECTIVE please – even the young have odds of 1: 2000 of death every year due to all causes. [REF US CDC]
You may also like;










 All products bought through EnrichLife.co come with a 30-day MONEY BACK GUARANTEE
All products bought through EnrichLife.co come with a 30-day MONEY BACK GUARANTEE 
